 User Guide — Medication Reconciliation
User Guide — Medication Reconciliation
athenaOne for Hospitals & Health Systems
When a patient is admitted, transferred, and discharged, all active medications must be reconciled, to create a "reconciled medications list." You can reconcile medications from within the hospital chart Medications section, and from Order Entry for admission, transfer, and discharge orders.
When you continue, substitute, or discontinue medications during the reconciliation process, athenaOne creates new medication orders to be signed by the provider.
Intrahospital transfers, such as transferring a patient from the ICU to a swing bed, are defined as a change in the level of care. For intrahospital transfers, the medication reconciliation should be performed by the receiving provider.
When a patient is admitted to the hospital, the Admission Note should be updated with all the medications that the patient had been taking at home.
The hospital chart Medication section lists the medications that the patient had been taking at home (from the list of home medications recorded in the Admission Note), as well as any medications that were ordered in the hospital. The provider can then use these two side-by-side lists to reconcile which medications should be continued during the hospital stay, to create a "reconciled medications list."
Upon an intrahospital transfer, from one level of care to another, the hospital chart Medications section lists only the current hospital medications. Upon transfer, the receiving provider can review and update the list of medications for the new level of care.
Upon discharge, the hospital chart Medications section again lists both the list of home medications and the current hospital medications list. The attending provider can review both lists, and create a new reconciled list of medications to be continued when patient leaves the hospital.
- You can find the Reconcile home medications link in the Medications tab of the patient chart, under Active Medications:
Click the
and in Order Entry:
Click the Reconcile home medications link to display the Medication Reconciliation window: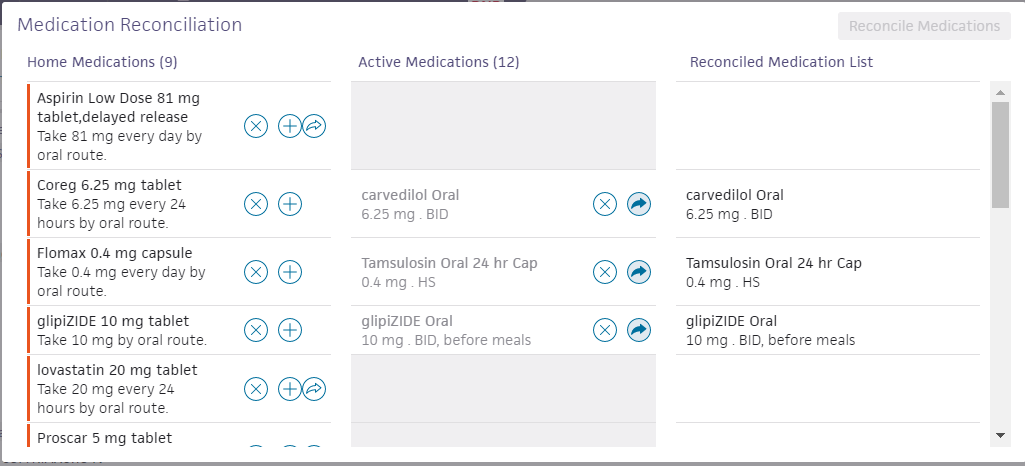
- For each home medication listed, you can:
- Click the X icon
 to discontinue the medication during the hospital stay.
to discontinue the medication during the hospital stay.
Discontinued medications remain on the patient's pre-admission and will be available during the discharge medication reconciliation process. - Click the arrow icon
 to continue the medication during the hospital stay.
to continue the medication during the hospital stay.
Continued medications appear in the Reconciled Medication List in the right side.
The medication's sig is automatically converted to an inpatient medication order.
If the medication is not available in the hospital pharmacy, the following message appears: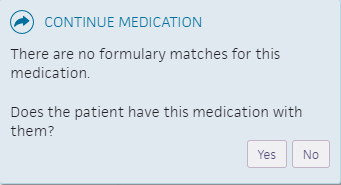
- If the patient does not have the medication with them, you can click the plus icon
 to add a substitute medication for the duration of the hospital stay. A substitute medication replaces one that is not available from the hospital pharmacy.
to add a substitute medication for the duration of the hospital stay. A substitute medication replaces one that is not available from the hospital pharmacy.
- Click the X icon
-
After all medications have been acted upon, click Reconcile Medications.
- From Order Entry, complete the sig and other required fields.
For substituted medications, if the patient's own medication will be used, select the checkbox. - Click Sign Orders.
After an order is signed, it appears in Order View. The consulting physician will receive notification that there is an open consult order.
- You can find the Review medications upon transfer link in the Medications tab of the patient chart, under Active Medications:
and in Order Entry:
Click the Review medications upon transfer link to display the Medication Reconciliation window: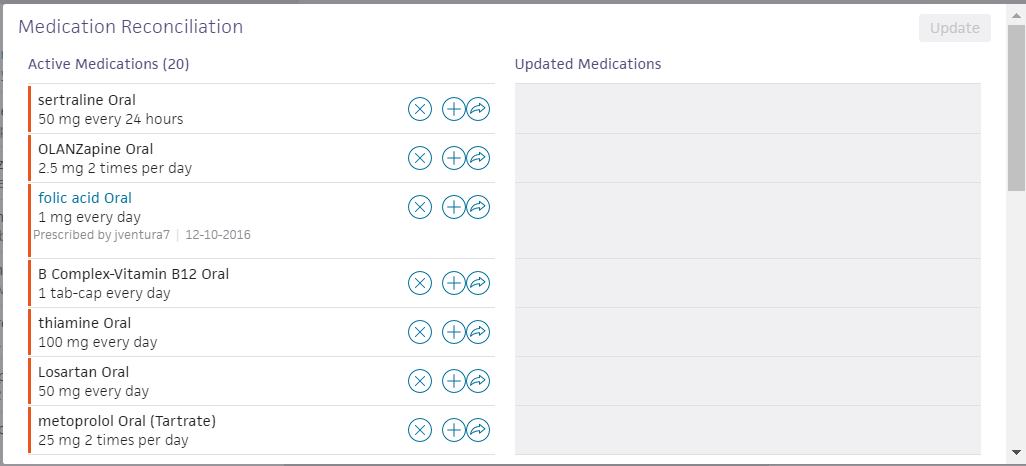
- For each active medication listed, you can:
- Click the X icon to discontinue an active medication upon transfer.
- Click the arrow icon to continue the medication after the transfer.
Continued medications appear in the Updated medications appear on the right side. - You can click the plus icon to add a substitute medication when the patient is transferred. Enter the same sig information for the substitute medication.
- Click the X icon
-
After all medications have been acted upon, click Reconcile Medications.
- From Order Entry, complete the sig and other required fields for any ordered and substituted medications.
- Click Sign Orders.
After an order is signed, it appears in Order View.
As part of the discharge process, nurses can enter diagnoses and orders, and reconcile medications if given a verbal order to do so by the ordering physician. Only physicians can sign orders.
- Display the patient's Discharge tab: In the patient chart, click the arrow in the green workflow menu (at the upper right) and select Go to Discharge. (The options available in the green workflow menu depend on your user role.)
- Click Post-Discharge Orders.
- Order Entry — Search for and select orders. If given a verbal order, a nurse can search for and select orders.
Tip: To order referrals, search for "referrals" and include summaries of care. You can search for "after your visit" to locate patient education orders.
Note: Some order types may require a diagnosis. -
To mark an order as not given, click Not Given when, for example, the patient refused the order, or a medication wasn't available. This action ensures that quality measures are not affected negatively.
You must then select a reason for not giving the order.
You can also include a note to the patient and an internal note.
Orders marked as Not Given are listed in the Medications Not Given section of the Discharge Summary, but not in the medication list or the Patient Portal. This ensures that the patient does not accidentally view an order or take a medication that was explicitly refused.
Reconcile the medications list
- If the Reconcile medications for discharge link is visible, click this link to review the patient's home and inpatient medications.
The patient's home medications are listed on the left, inpatient medications are listed in the center, and the discharge medication list appears on the right. - For each medication on the list, use the arrow icon to indication continue or use the X icon to discontinue upon discharge. The list of home medications marked continue produces the Discharge Home Medications list.
- Click Reconcile Medications to create the Discharge Home Medications list.
(All medications in the list must be acted upon before the button appears green.) - Discharge Home Medications — Review the list of medications to be continued upon discharge. Click a medication to view or edit the details, or to remove it from the list.
Note: In the patient's chart, the medications flowsheet will reflect the changes made when medications are reconciled.