 User Guide — athenaClinicals Care Plan
User Guide — athenaClinicals Care Plan
To help a patient prevent or better manage an illness, care managers can create a care plan in athenaClinicals. A care plan helps you manage care-related events and goals for an individual patient.
In the patient chart:
- Click the Care tab on the left side of the page.
- Under Active Plans, click the view more icon
 next to Open Care or Treatment Plan.
next to Open Care or Treatment Plan. - In the active plan workspace that opens, click the Care Plan tab to access an active plan or add a new plan.
To display an existing care plan for a patient from the patient briefing, click Go to Care Plan.
To access the patient care plan, you must have the Clinicals: Edit Chart role or permission.
You can create a personalized care plan in which you select problems, goals, and tasks individually.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Click Add Care Plan. A blank care plan opens.
- Health Concerns — Select the problems, barriers to care, or social determinants of health that the patient should focus on with guidance and assistance from the patient's care team. These may be unrelated to the health problems listed in the Problems section of the patient chart.
- Health status — Select the status that best describes the patient's overall health.
Note: Health statuses are backed by standard SNOMED-CT codes for data interoperability. - Clinical Care Management Events — Click
 to document a care management event. These events are narrative summaries of each patient interaction.
to document a care management event. These events are narrative summaries of each patient interaction. - Clinical Goals — Click to search for a goal, or you can enter a free-text goal in the search field. You can add multiple goals.
- All Patient Tasks — Click to search and select a task, and then enter instructions for the patient in the Instructions field. The patient is responsible for these tasks to accomplish their goals.
- All Care Team Tasks — Click to search and select a task, and then enter instructions for the care team in the Instructions field. The care team is responsible for these tasks to help patients achieve their goals.
After you create a care plan, you can add templated information for a number of common chronic conditions. Using a template, you can quickly enter a set of goals, tasks, and assessments commonly associated with a condition into the default care plan you created. For more details on the available templates, see Care Plan Templates.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Click Apply Templates next to the Clinical Goals section title.
- Care plan templates — Select one or more care plan templates. Start typing the name of a template to search for and select it.
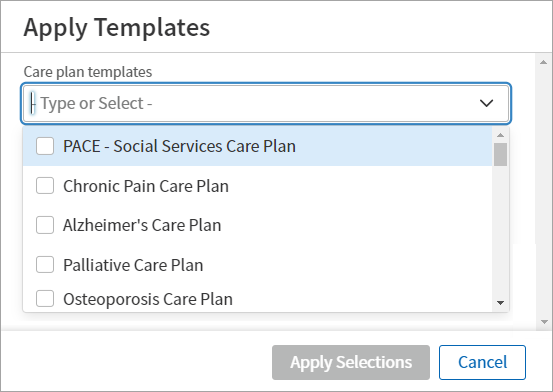
- Select or deselect content groups or individual options for each template.
- Click Apply Selections.
- Enable full-screen view — Click the Care tab to enable the full-screen view. To disable the full-screen view, click the Care tab again.
- Collapse side panel — If you want to focus more on items in the right panel of the care plan (such as patient goals), you can collapse the left panel of the care plan by clicking Hide Panel. To re-open the left panel, click Show Panel.
- Switch between chart elements — Typically, care managers and clinicians complete work in the care plan while also performing work elsewhere in the patient chart. You can easily switch between viewing the care plan and viewing a CCDA document or patient case. To hide the care plan behind another open chart element, click Send Care Plan to Back. To open the care plan in front of another open chart element, click Bring Care Plan to Front.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- In the Care Plan Summary section, click Remove Plan.
- Reason for removal — Document the reason you are archiving the care plan.
- To permanently delete the care plan, check the box next to Added in Error (delete). Deleting a care plan cannot be undone.
- Click Remove Plan. The plan is moved to an archived state within the Historical tab.
Note: In the Care tab, click Historical to access the patient's archived care plans.
In the Care Plan Summary section, select the desired review date in the Date of next review field. The plan updates automatically.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- In the Care Plan Summary section, click Create Plan CCDA.
- Send to — Enter the facility where you are sending the hospital care plan.
- Method — Select Paper print-out or AthenaFax.
- Attention — Optionally, enter the person at the facility who should receive the care plan.
- Note — Optionally, enter a note about the care plan for the person receiving the document.
- Select the Submit option.
- Click Save.
- Click
 Print.
Print.
A print preview of the document appears. - Click the print icon at the top right of the print preview.
- Select your printing options.
- Click Print.
Occasionally, more than one member of a patient's care team may attempt to update a section of the patient care plan at the same time. When a conflict occurs, athenaOne displays a warning message with a Refresh button (the button name depends on the section of the care plan being edited, for example, "Refresh Goals").
Click Refresh to refresh the section content and continue your edits. The other care team member will then see the section of the care plan as it currently exists, with any changes you made.
The audit history shows all information that was added or edited in the patient care plan, along with the username of the person who added or edited the data and the date and time of the updates.
- Display the Chart Export page: In the patient chart, click the Menu icon
 and select Chart export.
and select Chart export.
The Chart Export window appears. - In the Chart Sections area, under Available Attachments, select Care Plan Audit and click the right arrow icon
 to move the audit to the Selected Attachments column.
to move the audit to the Selected Attachments column. - Click Export Chart Sections.
A document containing the care plan is displayed.
Health concerns documented in the care plan are problems, social determinants, or barriers to health that patients should focus on with guidance and assistance from the patient's care team.
- Problem — Any diagnosis or problem that necessitates follow-up and monitoring in the care plan.
Examples: pregnancy, diabetes - Barrier to care — Any factor that may prevent a patient having access to the health care services.
Examples: homeless, financially poor, difference in location - Social determinant of health — Any condition of the patient's life or environment that may affect their access to health care services.
Examples: In debt, victim of abuse, low-level literacy
Not all problems documented on the Problems tab need to be addressed in the care plan as health concerns.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Click next to Health Concerns.
- Search for and select a health concern from the SNOMED library.
- Notes — Provide additional context about the health concern.
- Link to existing goals — Select from related goals that you added in the Goals section of the care plan.
- Click Add.
Edit or delete a concern
Click the menu  to the right of a concern. Click Edit Health Concern or Delete to update or permanently delete it.
to the right of a concern. Click Edit Health Concern or Delete to update or permanently delete it.
Update the status of a concern
Click the menu to the right of a concern. Select Make Inactive to update the status. You can change the status back to Active at any time. To reactivate, click the menu to the right of the concern and select Make Active.
Access inactive concerns
Click the Show filter  to the right of the Health Concerns section title. In the filter menu, select Inactive. Remove the selection from Active to view only inactive concerns, or select both options to view all.
to the right of the Health Concerns section title. In the filter menu, select Inactive. Remove the selection from Active to view only inactive concerns, or select both options to view all.
Care management events are narrative summaries of each patient interaction. Event types include Documentation, Office Visit, and Phone Call.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Click next to Clinical Care Management Events.
- Event date and time — Select or enter the date and time for the event.
Note: athenaOne displays the current date by default. - Event type — Select the event type from the menu: Documentation, Office Visit, or Phone Call.
- Duration (optional) — Enter the amount of time spent on the event. athenaOne totals the time entered in the Duration field to come up with a monthly total that appears in the Care Plan Report.
- Summary — Enter a summary of the event (for example, "Discussed diet with patient").
- Click Add Event.
Click the menu to the right of a care management event. Click Edit Event or Delete to update or permanently delete it.
Goals are targets for patients in care management. Specific to a patient's situation, goals focus on a desired outcome. Care managers can document a desired result or possible outcome that a patient commits to with the care manager.
You can search for and select goals in the clinician-curated content library or create custom goals for the patient.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Click next to the Clinical Goals section title.
- Patient goal statement — Enter details explaining why, in the patient's words, the patient is committed to this goal.
- Goal title — Search for and select a global goal, or enter the goal in your own words.
- Add Goal Description — Click to reveal the Goal Description field and enter details about the desired outcome for this goal. If you select a global goal in the Goal title field, this field populates automatically.
- Targeted health concerns — Select one or more existing health concerns that the goal is addressing. (You can also form this association when creating or editing a health concern.)
- Goal priority — Select a priority value for the goal. This field is useful for patients with multiple conditions or for goals that should be met in sequential order.
- Click Add.
When you add a goal or update an existing goal in the care plan, you can use the Make It Measurable section to select a qualitative measurement (default) or a quantitative clinical measurement (for example, hemoglobin A1c results). You can record a baseline value, milestones, and additional details.
Add a qualitative measurement
- Add a new goal or edit and existing goal. Scroll down to the Make It Measurable section.
- Measurement type — Select Qualitative.
- Baseline description — Describe the patient's initial status with respect to the goal.
- Goal start date — Enter or select a start date for the goal.
- Goal target date — Select a preset or custom due date for the goal, or leave the default setting (No Target Date) selected.
- Click Add.
Add a quantitative measurement
- Add a new goal or edit and existing goal. Scroll down to the Make It Measurable section.
- Measurement type — Select a clinical measurement type.
- Select Add from patient's chart to populate the patient's three most recent clinical values (based on the selected measurement type) as options in the Baseline value menu. To add data manually, click Add new.
Note: If there are multiple charts for one patient, athenaOne displays the three most recent clinical values across all patient charts. - Baseline value — Enter or select the patient's baseline value.
- Goal start date — Enter or select a start date for the goal.
- Goal target value — Enter or select the patient's target value.
- Goal target date — Select a preset or custom due date for the goal, or leave the default setting (No Target Date) selected.
- Add Milestones (optional) — Add one or more milestones to indicate incremental progress toward the goal's target value and date.
- Click Add.
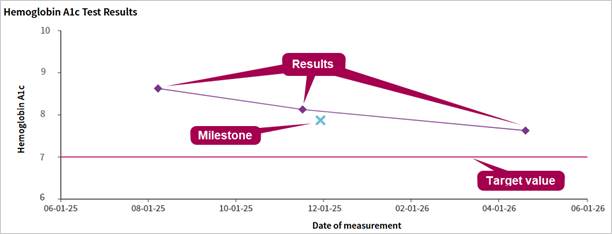
Visualize a patient's progress
Once you begin measuring a clinical data point, you can visualize the patient's baseline value, target value, and milestones against recorded clinical data in the patient's chart.
In the expanded view of the goal, athenaOne displays the relevant data in a line chart, allowing you to see at a glance how the patient is progressing toward the goal. To view the chart, locate the goal and click Show More.
Click the menu to the right of a goal to select an action.
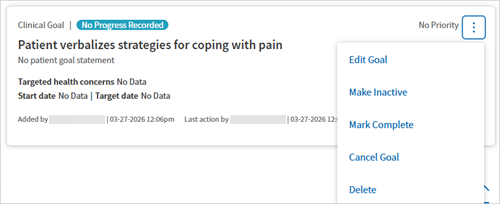
- Edit — Opens the goal for editing.
- Make Inactive — Updates the state of a goal to Inactive, so you can filter it out of active goals if desired. This option is useful for goals not currently being worked on by your patient.
- Complete — Updates the state of a goal to Complete, so you can filter it out of active goals if desired.
- Cancel — Updates the state of a goal to Canceled, but does not permanently delete it. This is useful when reviewing goals you and your patient consider no longer relevant.
- Delete — Permanently removes goals entered in error.
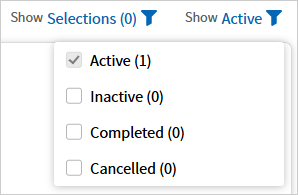
Access inactive, completed, or canceled goals
Click the Show filter to the right of the Clinical Goals section title. In the filter menu, select the states to view, which includes options to view Active, Inactive, Completed, or Cancelled goals. Select all states to access all goals.
View goals by linked health concerns
Click the Show Selections filter to the right of the Clinical Goals section title. In the filter menu, select one or more linked health concerns.
You can select a goal progress status to indicate how the patient is progressing towards achieving a goal. You can also enter a justification for the change and view a summary of changes and rationale.
- In the lower right corner of a goal, click Show More. Initially, the goal progress status appears as NO PROGRESS RECORDED by default.
- Click
 next to Goal Progress Status.
next to Goal Progress Status. - Work with your patient to determine the status of their goal. Select an option closest to the status of the goal as they would describe it.
- Enter a note with information the patient shares about their progress. Click Record Progress.
- The most recent update appears beneath the status entry field. To view all entries, click Show Progress History.
There are two types of tasks in the care plan: Patient Tasks and Care Team Tasks.
- Patient Tasks — Patient tasks are assignments in a care plan for the patient, such as, "Take your blood pressure." The patient is responsible for these tasks to accomplish their goals. You can search for and select patient tasks in the clinician-curated content library, and you can create custom tasks for the patient.
-
Care Team Tasks — Care team tasks are assignments that the care team is responsible for to help patients achieve their goals, such as "Share diabetes education content with patient." You can use the care team tasks as a reminder or to-do list for the next time a care manager reviews the patient's care plan.
You can search for and select patient and care team tasks in the clinician-curated content library, and you can create custom tasks. You can associate a task with an active goal either by selecting the goal in the Associate to active goal field or by creating the task directly within a specific goal.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- In the lower right corner of a goal, click Show More.
- Click next to Patient Tasks or Care Team Tasks.
- Task title — Search for and select a global task, or enter the task in your own words.
- Instructions — Provide criteria for task completion.
- Start date and Target date — Select a start date and target date for the task. Click Date Range to toggle the date range off and leave the start and target dates undefined.
- Click Add. The task appears both with the associated goal and in the All Patient Tasks or All Care Team Tasks sections of the care plan.
Note: To create standalone tasks, click ![]() next to All Patient Tasks or All Care Team Tasks. In this case, you can choose to associate the task with a goal later using the Associate to active goal field.
next to All Patient Tasks or All Care Team Tasks. In this case, you can choose to associate the task with a goal later using the Associate to active goal field.
You can record multiple progress updates on a patient or care team task and complete it when ready. This is ideal for tasks that require regular updates.
- In the patient chart, click the Care tab, open the plan under Active Plans, and select the Care Plan tab.
- Locate the task and click Record or Show More.
- In the Record Task Progress section, select or enter the appropriate value and complete the fields:
- Date of occurrence — Select a date (required) and time (optional) to specify when you logged a task or when the task was completed. The fields default to the current date and time.
- Task requirements — Select Met or Not Met. This field appears for tasks in which you document whether or not the patient satisfied the task requirements.
- Note (optional) — Enter additional information about the task.
- Save the progress record:
- Click Add recording to save the progress record and keep the intervention active.
- Click Record and Complete to save the progress record and complete the intervention at the same time.
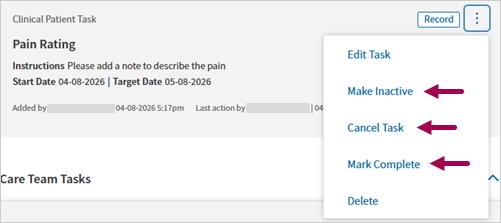
and select Mark Complete.
Edit or delete a task
Click the menu to the right of the task. Select Edit Task or Delete to update or permanently remove it.
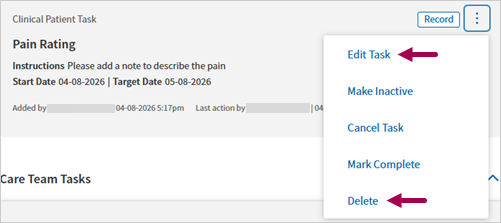
Update the state of a task
Click the menu to the right the task. Select Make Inactive, Cancel Task, or Mark Complete to update the state. You can change the state of a task to any other state, including Active, at any time.
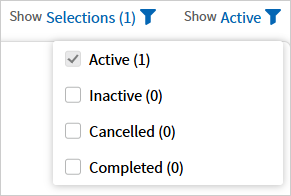
Access inactive, completed, and canceled tasks
Click the Show filter to the right of the task section title. In the filter menu, select the states to view. Select all states to access all tasks.
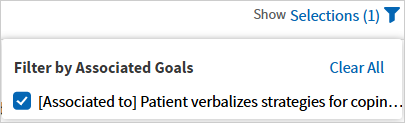
View tasks by associated goals
Click the Show Selections filter to the right of the All Patient Tasks or All Care Team Tasks section title. In the filter menu, select one or more associated goals.
The goals and tasks included for a chronic care diagnosis or program come from a clinician-curated content library that we've built with a focus on identifying clear and helpful goals that relate to the diagnoses and tasks that help achieve each goal.
For each chronic care diagnosis supported by athenaClinicals, a team of licensed clinicians at athenahealth has identified one or more goals and tasks that are commonly used by athenaClinicals users in association with the diagnosis.
You can remove goals and tasks from a care plan template that you add to a patient's care plan, but you cannot add or edit items in the template itself. If you add multiple care plan templates that share some of the same content (for example, "Weigh yourself weekly" may be a task for several conditions), the shared content is added only once in the care plan.
Templated care plan information is available for the following chronic conditions and programs supported by athenaClinicals.
- Acute Pain
- Alcohol Abuse
- Alzheimer's
- Anemia
- Anxiety
- Asthma
- Atrial Fibrillation
- Attention-Deficit/Hyperactivity Disorder (ADHD)
- Autism
- Bariatric Surgery
- Bipolar
- Cancer
- Chronic Fatigue Syndrome (CFH)
- Chronic Kidney Disease
- Chronic Migraines
- Chronic Obstructive Pulmonary Disease (COPD)
- Chronic Pain
- Chronic Post-COVID-19 Syndrome
- Cognitive Impairment
- Congestive Heart Failure (CHF)
- Coronary Artery Disease (CAD)
- COVID-19 Comprehensive
- Crohn's Disease
- Dementia
- Depression
- Diabetes Mellitus (DM)
- Drug/Substance Abuse
- End Stage Renal Disease (ESRD)
- Fall Risk
- Fibromyalgia
- Gastroesophageal Reflux Disease (GERD)
- General Surgery
- Gestational Diabetes
- Hearing Loss
- Hepatitus/Chronic Viral B&C
- HIV/AIDS
- Hyperlipidemia
- Hypertension (HTN)
- Hypothyroidism
- Impaired Skin Integrity
- Irritable Bowel Syndrome (IBS)
- Menopause
- Multiple Sclerosis (MS)
- Obesity
- Obstructive Sleep Apnea
- Osteoarthritis
- Osteopenia
- Osteoporosis
- PACE - In-Home Services
- PACE - Nursing
- PACE - Social Services
- Palliative
- Parkinson's
- Pediatric Attention-Deficit/Hyperactivity Disorder (ADHD)
- Pediatric Cerebral Palsy (CP)
- Pediatric Oppositional Defiant Disorder (ODD)
- Pediatric Osteopenia
- Pediatric Recurrent Otitis Media
- Peripheral Vascular Disease (PVD)
- Prediabetes
- Posttraumatic Stress Disorder (PTSD)
- Recurrent Pneumonia
- Rheumatoid Arthritis
- Seizure/Epilepsy
- Stroke
- Transitions of Care
- Type 1 Diabetes
- Type 2 Diabetes