 User Guide — Nurse Workflow (Emergency Department)
User Guide — Nurse Workflow (Emergency Department)
athenaOne for Hospitals & Health Systems
Table of Contents
Patient registration and check-in
To discharge a patient from the emergency department
Workflow overview
Registration (nurse) or staff)
Either a member of the registration or nursing staff handles the registration process of the patient.
Once registered, the patient's name appears at the bottom of the Tracking Board, under the waiting room section. If a chief complaint was entered during registration, it appears in the Chief Complaint column of the Tracking Board.
Triage (nurse)
During triage, you enter or update the chief complaint, assign acuity, place the patient into a treatment or trauma room, and sign the triage note. This information is displayed on the Tracking Board, and the patient's name moves to the top section of the Tracking Board.
Next, you perform an initial assessment and document any history and findings.
The patient is now ready for the physician.
Provider Assessment (physician)
The physician performs the Provider Assessment using a navigation bar with six sections: Review, ROS, HX, PE, A&P, and Sign-off.

The information entered during registration, triage, and initial assessment (medications, histories, allergies, etc.) is available for the physician to review within the Provider Assessment.
Additional orders, notes (physician)
After the physician completes the Provider Assessment, the physician can enter additional orders and notes.
Discharge or transfer
Either you or the physician can create the Discharge Plan. The physician signs the discharge orders and creates the ED course. As part of the Discharge plan, you can enter the discharge instructions, and create and sign the nursing care plan.
Patient registration and check-in
- On the Main Menu, click Patients. Under Patient Registration, click New Hospital Visit.
- Use the search fields to search for the patient record.
- If the patient record is found, click the patient name and then click New ER Visit.
- If the patent record is not found, click Create visit for a new patient, and then click New ER Visit.
- To register an unidentified patient, select the Patient identity cannot be determined option (at the top of the New ER Visit window) and complete the estimated information fields. You can update the patient's demographic information on the Visit - Patient Access page on the Registration tab, or on the Quickview, or Patient Registration page when the information becomes available.
When you enter an estimated age, athenaOne populates the Estimated DOB field.
The Race and Ethnicity fields are not required.
A notification appears at the top of the Quickview page, the full Registration page, and on the Visit - Patient Access page on the Registration tab to indicate that the patient is registered as an unidentified patient. - Enter any available patient demographic information in the fields provided.
- Enter the visit details in the fields provided.
Note: The chief complaint you select will appear on the Tracking Board and in the patient chart briefing. - Check any notices on file.
- Click Check in Patient.
The Tracking Board
The Tracking Board appears when you first log in to an emergency department that uses athenaOne for Hospitals & Health Systems. The Tracking Board is the starting point for the ED physician workflow and provides direct access to patient charts.
The top of the Tracking Board lists all the rooms in the emergency department, with the patients currently assigned to each room. The lower section lists the patients checked in to the emergency department waiting room.
These Tracking Board columns provide quick insight into patient status:
STATUS
The patient's status: Triage, Discharging, or Transferring. If no status is recorded, the cell is blank.
ALERTS
The patient's allergies, and 72-hour alerts, populated from the patient's precautions list in the Diagnoses section of the patient chart.
VITALS
The last time the patient's vitals were recorded. You can pause your cursor over the vitals to see the vital readings.
These columns show the status of the patient's ordered tests and medications:
LAB
Click the icon to access the patient's lab orders in the Results section of the patient's chart.
![]() — Lab orders are placed, and all results are returned.
— Lab orders are placed, and all results are returned.
![]() — Lab orders are placed, and some results are returned.
— Lab orders are placed, and some results are returned.
![]() — Lab orders are placed, and no results are returned.
— Lab orders are placed, and no results are returned.
IMG
Click the icon to access the patient's imaging orders in the Results section of the patient's chart.
![]() — Imaging orders are placed, and all results are returned.
— Imaging orders are placed, and all results are returned.
![]() — A returned imaging order is critical.
— A returned imaging order is critical.
![]() — Imaging orders are placed, and no results are returned.
— Imaging orders are placed, and no results are returned.
ORD
Patient's orders.
You can click the link to view the orders list in the patient's chart.
A plus icon ![]() indicates there are no orders for this patient.
indicates there are no orders for this patient.
You can click the plus icon ![]() to add orders directly to the patient's chart.
to add orders directly to the patient's chart.
MED
Patient's medications.Click the link to view the medications list in the patient's chart.
Triage Note
You perform the emergency department triage and record the information in the triage note.
- Display the Tracking Board: Click the athenaOne logo in an emergency department that uses athenaOne for Hospitals & Health Systems.
- On the Tracking Board, click a waiting patient's name.
The patient chart appears. - On the patient's chart, click the arrow in the green workflow menu (at the upper right) and select Start Triage. (The options available in the green workflow menu depend on your user role.)
Note: If triage had been started, the menu will say Continue Triage.
- Chief Complaint — Click the plus icon
 to search for and select a chief complaint.
to search for and select a chief complaint. - Acuity — Select the level of acuity.
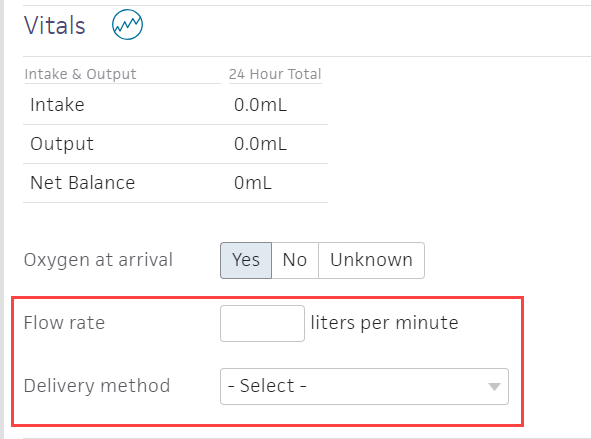
- Vitals — Click the flowsheet icon
 to record vitals. This field may be populated automatically with information previously recorded in the patient chart.
to record vitals. This field may be populated automatically with information previously recorded in the patient chart.
Note: The Include vitals in summary box is unchecked by default, but you can check this to include the latest vitals in the summary of the triage note. - Oxygen at arrival — If you click Yes, enter the flow rate and select the oxygen a delivery method
- Home Medications — Click the plus icon
 to search for and select home medications.
to search for and select home medications.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Allergies — Click the plus icon to search for and select allergens.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Nursing Assessments — Enter a free-text assessment, or click the plus icon to search for and select an assessment template where you can record information.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Click Sign-off or click Next.

- Click Sign Note. The triage note appears in the Recent Notes section of the patient briefing and in the Notes section of the patient chart.
Note: The timestamp appears just below the Sign Note button.
You can click the timestamp to update the date and time, provided that the date you enter is within 30 days of the current date. When you update a timestamp, the note is marked "Late entry."
Initial assessment
You perform the initial assessment of the patient, and record the information. Physicians will review the information you enter in the triage note and initial assessment.
- On the emergency room Tracking Board, click the patient's name.
The patient chart appears. - On the patient's chart, click the arrow in the green workflow menu (at the upper right) and select Start Initial Assessment. (The options available in the green workflow menu depend on your user role.)
The Assess step is highlighted in the navigation bar.

- Nursing Assessments — You can enter a free-text assessment in the text box, or you can click the plus icon to search for and select an assessment template to record the information.
- Click Next in the upper right corner, or click Hx in the navigation bar at the top of the page.

- Problems — Click the plus icon to search for and enter patient problems.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Surgical History — Click the plus icon to search for and enter surgical history.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Home Medications — Click the plus icon to search for and enter home medications.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Allergies — Click the plus icon to search for and enter allergens.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Vaccines — Click the plus icon to search for and enter vaccines.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Family History — Click the plus icon to search for and enter vaccine information.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Social History — Click the plus icon to search for and select social history information.
Complete the smoking status fields.
Note: This field may be populated automatically with information previously recorded in the patient chart. - Click Next in the upper right corner, or click Orders in the navigation bar at the top of the page.

- Order Entry — Click the plus icon to search for and select orders.
Enter the sig for each order in the fields provided.
Check the boxes for each order that you want to enter (nurse) or sign (physician). - Click Enter Orders (nurse) or Sign Orders (physician).
- Click Next in the upper right corner, or click Sign-off in the navigation bar at the top of the page.

- Summary — Review the information recorded under each heading.
- Click Sign Note.. The initial assessment appears in the Recent Notes section of the patient briefing and in the Notes section of the patient chart.
The Discharge Plan and patient disposition
After the patient is seen and is ready to leave the ED, the physician can either discharge the patient or transfer the patient to inpatient or surgery.
As part of the Discharge plan, you can complete the discharge instructions, and create and sign the nursing care plan.
The physician must sign the Discharge Plan.
To discharge a patient from the emergency department
- Display the Tracking Board: Click the athenaOne logo in an emergency department that uses athenaOne for Hospitals & Health Systems.
- On the Tracking Board, click a patient's name.
The patient chart appears. - In the patient chart, click the arrow in the green workflow menu (at the upper right) and select Go to Discharge Plan. (The options available in the green workflow menu depend on your user role.) Alternatively, in the patient chart, click the Discharge chart tab at the left side of the page.
Record discharge order information
- Click Discharge Order.
- Ordering physician — Select the ordering physician. (This field appears for nurses only.)
- Final diagnosis — Search for and enter a final diagnosis.
- Condition — Enter the patient's condition the time of discharge.
- Disposition — Select the disposition of the patient after discharge.
Enter discharge orders
- Click Post-Discharge Orders.
- Order Entry — Search for and select orders. If given a verbal order, a nurse can search for and select orders.
Tip: To order referrals, search for "referrals" and include summaries of care. You can search for "after your visit" to locate patient education orders.
Note: Some order types may require a diagnosis. -
To mark an order as not given, click Not Given when, for example, the patient refused the order, or a medication wasn't available. This action ensures that quality measures are not affected negatively.
You must then select a reason for not giving the order.
You can also include a note to the patient and an internal note.
Orders marked as Not Given are listed in the Medications Not Given section of the Discharge Summary, but not in the medication list or the Patient Portal. This ensures that the patient does not accidentally view an order or take a medication that was explicitly refused.
Reconcile the medications list
- If the Reconcile medications for discharge link is visible, click this link to review the patient's home and inpatient medications.
The patient's home medications are listed on the left, inpatient medications are listed in the center, and the discharge medication list appears on the right. - For each medication on the list, use the arrow icon to indication continue
 or use the X icon
or use the X icon  to discontinue upon discharge. The list of home medications marked continue produces the Discharge Home Medications list.
to discontinue upon discharge. The list of home medications marked continue produces the Discharge Home Medications list. - Click Reconcile Medications to create the Discharge Home Medications list.
(All medications in the list must be acted upon before the button appears green.) - Discharge Home Medications — Review the list of medications to be continued upon discharge. Click a medication to view or edit the details, or to remove it from the list.
Note: In the patient's chart, the medications flowsheet will reflect the changes made when medications are reconciled.
Enter discharge instructions
- Click Next or click Instructions in the navigation bar at the top of the page.

- Nursing Summary of Care — Enter the nursing summary of care.
- Patient Goals — Enter the patient goals.
- Patient Instructions — Enter the patient instructions.
- Portal Registration — You can register the patient for the Patient Portal, if the patient consents.
Note: After discharge, patients registered for the Patient Portal can access their summary of care record on the My Health page of the Patient Portal. - Click Enter Instructions.
Review and add letters
- Letters — Click the Letters plus icon to display the Add Letter form, complete the fields provided, and select a delivery option.
If the patient has Patient Portal access, you can select Close and Email Patient. athenaOne may close certain Patient Care Summaries when you sign and approve them, so they do not appear in the Clinical Inbox unnecessarily.
Note: athenaOne automatically generates and sends the Summary of Care Record (SCR) via DIRECT to the Primary Care Physician (PCP) and Receiver Facility on record when you complete discharge and click Discharge Complete. The patient can access the Summary of Care record on the My Health page of the Patient Portal. - Review the information under the Discharge Summary heading.
- Click Done to complete the Discharge Plan.
Note: The discharge plan stays open until all steps are signed.
After discharge, patients registered for the Patient Portal can access their summary of care record on the My Health page of the Patient Portal. - After the patient leaves the hospital, on the patient briefing, enter the date and time that the patient left, and click Discharge Complete to close the stay. This removes the patient from the Patient List (or Tracking Board).

Note: If the patient has Patient Portal access, athenaOne automatically moves signed Patient Information orders and Patient Care Summaries from Review status to Notify by Portal status, and to Close status for other patient correspondence.
If the patient does not have Patient Portal access and the Paper option is selected in the Patient care summary and patient letter delivery preference field (under the Registration Information heading) on the Quickview, you should select Close manually.
To enter a transfer order from emergency to surgery
- Click the patient's name on the Tracking Board to display the patient's chart.
- In the patient chart, click the arrow in the green workflow menu (at the upper right) and select Add Patient Transfer. (The options available in the green workflow menu depend on your user role.)
- Transfer date and time — Enter the date and time for the transfer.
Tip: You can enter "now" in the time field to input the current time and date, or you can enter "t" in the date field for the current date. - Transfer reason — Enter the reason for transferring this patient.
- Attending physician — Select the attending physician who is ordering the transfer.
- Department — Select the receiving surgery department.
- Level of Care — Select the level of care to be provided.
- Service — Select the service to be provided to the patient.
- Telemetry — Click Yes, No, or Remote.
- Condition — Select the patient's condition.
- Precautions — Click the plus icon to add a precaution.
- Click Enter Transfer (nurse) or Sign Transfer (physician).
The patient status (at the top of the patient briefing and on the Tracking Board) shows that the patient is transferring.
The patient's name is added to the surgery department's Patient List with a status of Checked in.
Record that the patient has departed the emergency department
- At the top right of the patient briefing, enter the time and date the patient departed the emergency department.

Tip: You can enter "now" in the time field to input the current time and date, or you can enter "t" in the date field for the current date. - Click Mark as Departed.
Note: You can delete a transfer order that was not entered by a provider, as long as it has not yet been signed by a provider. You can cancel a transfer order (signed or unsigned) if a provider has not yet marked the patient as "Arrived" in the new department. To delete or cancel transfer orders, you must have the Inpatient Clinicals: Transfer/Discharge Sign-off permission.
To enter a transfer order from emergency to inpatient
From the Emergency or surgery department
- In the Patient List, click the patient's name to display the briefing.
- In the patient chart, click the arrow in the green workflow menu (at the upper right) and select Go To Admission Order. (The options available in the green workflow menu depend on your user role.)
- Admission date and time — Enter the time and date of admission.
Tip: You can enter "now" in the time field to input the current time and date, or you can enter "t" in the date field for the current date. - Department — Select the admitting or receiving department.
- Admitting physician — Select the admitting physician.
- Attending physician — Select the attending physician.
- Service — Select the service.
- Telemetry — Click Yes, No, or Remote.
- Level of care — Select the level of care.
- Primary diagnosis — You can click the plus icon to add a diagnosis, or click the X icon
 to delete a diagnosis.
to delete a diagnosis. - Condition — Select the patient's condition.
- Precautions — You can click the plus icon to add a risk, or click the X icon to delete a risk.
- Expect patient to be discharged or transferred within 96 hours — Click Yes or No.
- Elective admissions — Click Yes or No.
- Enrolled in clinical trial — Click Yes or No.
- Click Sign Order.
The patient appears in the Patient List of the inpatient department as "Transferring from Emergency." - In the Patient List, click the patient's name to display the briefing.
- Time of departure — Enter the departure time and click the calendar icon
 to select the departure date.
to select the departure date. - Click Mark as Departed.
Note: For reporting purposes, the clock stops on the patient's total ED length of stay.
From the Inpatient department
- In the Patient List, click the patient's name to display the briefing.
- Time of arrival — Enter the arrival time and click the calendar icon to select the arrival date.
- Click Mark as Arrived.